






119 – EB2026 – PLANHO CONSULTORES. S.L.P. , PROFESSIONAL LIMITED COMPANY & 4B CONSULTANȚĂ ARHITECTURĂ S.R.L.
Autori principali: PLANHO (architects) Enrique Vallencillos Segovia, Manuel Perez Hernandez
Coautori: Mara Victoria Vergu-Bogoescu, Matei Bogoescu, Radu Costăchescu, Tudor Costăchescu
Colaboratori arhitectură: Alfonso Fernandez Sanchez, Alejandro Vallencillos Portillo, Ildefonsa Rodrigues Martinez
Colaboratori specialități: Andrei Aioanei
Asociere:
PLANHO CONSULTORES. S.L.P. , PROFESSIONAL LIMITED COMPANY 50%
4B CONSULTANȚĂ ARHITECTURĂ S.R.L. 50%


GENERAL INTRODUCTION
Hospitals are the most complex of the building types. Their constant functional and physical adaptation over time, due to the technological renewal of equipment and facilities, the dynamics of care management models and the changing demands of professionals and users, increases this complexity even further. Good hospital design must allow potential changes and extensions without compromising the efficiency of the daily medical activities.
Due to this complexity in form, function and evolution, considerable information has been published on how a hospital project should be approached. While there is no unique hospital model, key factors in choosing the best design option are size, range of services, sustainability and integration within the environment.
During our extensive practice in hospital design we found a recurring pattern common to all successful models, which is based on the fulfilment of two guiding principles:
The user (patient, medical staff and family) is the center of the system.
The building must be technically and functionally efficient.
The design of contemporary hospitals does not orbit exclusively around the needs of the doctors, architects or authorities, but takes into account all their users’ needs.
The hospitalization process is a source of severe stress for the patient, and therefore the quality of its environment is crucial, even more so when the patients are children, since their minds and body can be deeply affected during their visit or stay in the hospital.
In paediatric hospitals, special attention must be given to internal facilities and leisure spaces, playgrounds and educational areas for children and their families. This are complementary spaces, specific to the paediatric hospitals, which have unique physical characteristics.
Contemporary hospitals are more than just places for the provision of healthcare services. Usually they are the most important buildings in the city and the main point of reference for an entire society and time.
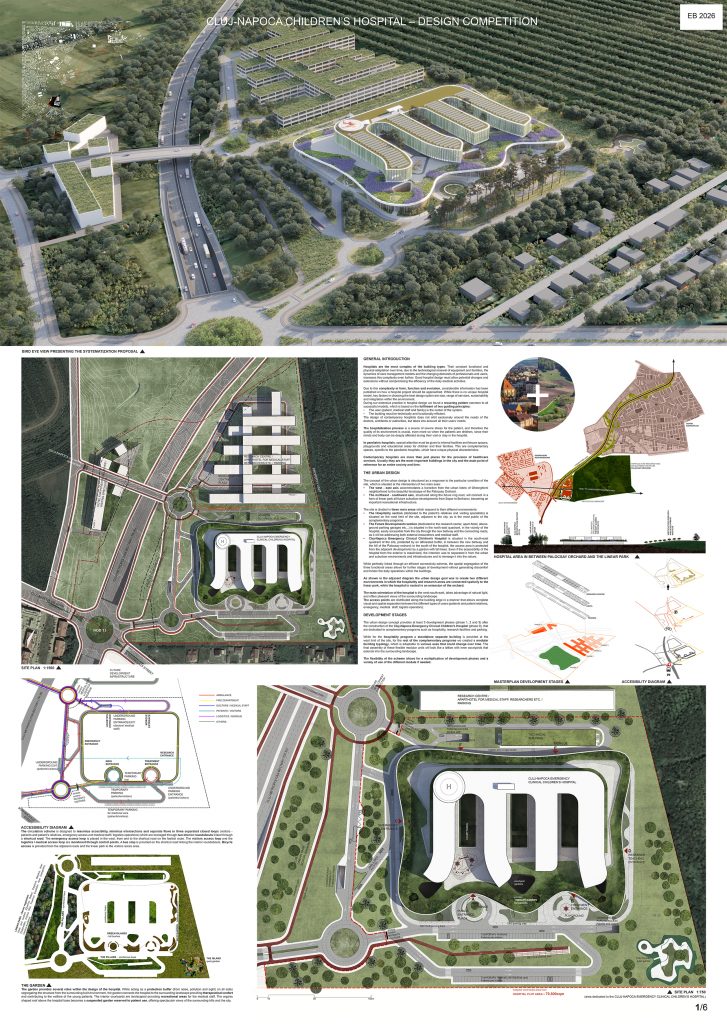
THE URBAN DESIGN
The concept of the urban design is structured as a response to the particular condition of the site, which is situated at the intersection of two main axes:
The west – east axis accommodates a transition from the urban fabric of Gheorghieni neighborhood to the beautiful landscape of the Palocsay Orchard.
The northeast – southwest axis, structured along the future ring road, will connect in a form of linear park all future suburban developments from Sopor to Borhanci, becoming an important recreational infrastructure.
The site is divided in three main areas which respond to their different environments:
The Hospitality section (dedicated to the patient’s relatives and visiting specialists) is situated on the west limit of the site, adjacent to the city, as is the most public of the complementary programs.
The Future Developments section (dedicated to the research center, apart-hotel, above-ground parking garages etc…) is situated in the north east quadrant, in the vicinity of the hospital, easily accessible from the city through the new beltway and the connecting roads, as it will be addressing both external researchers and medical staff.
Cluj-Napoca Emergency Clinical Children’s Hospital is situated in the south-east quadrant of the site, protected by an afforested buffer, in between the new beltway and the hill of the Palocsay orchard; to the south of the hospital, the access area is protected from the adjacent developments by a garden with tall trees. Even if the accessibility of the hospital from the exterior is maximized, the intention was to separated it from the urban and suburban environments and infrastructures and to immerge it into the nature.
While perfectly linked through an efficient connectivity scheme, the spatial segregation of the three functional areas allows for further stages of development without generating discomfort and hinder the daily operations within the buildings.
As shown in the adjacent diagram the urban design goal was to create two different environments in which the hospitality and research areas are connected spatially to the linear park, while the hospital is nested in an extension of the orchard.
The main orientation of the hospital to the west-south-east, takes advantage of natural light, and offers pleasant views of the surrounding landscape.
The access points are distributed along the building edge in a manner that allows complete visual and spatial separation between the different types of users (patients and patient relatives, emergency, medical staff, logistic operators).
DEVELOPMENT STAGES
The urban design concept provides at least 3 development phases (phase 1, 2 and 3) after the construction of the Cluj-Napoca Emergency Clinical Children’s Hospital (phase 0), that are dedicated to complementary programs such as hospitality, research facilities and parking.
While for the hospitality program a standalone separate building is provided at the west limit of the site, for the rest of the complementary programs we created a modular building typology, which is adaptable to various uses that could change over time. The final assembly of these flexible modular units will look like a lattice with inner courtyards that extends into the surrounding landscape.
The flexibility of the scheme allows for a multiplication of development phases and a variety of use of the different moduls if needed.
PROPOSED SCHEME
The main objective of our design proposal is to achieve the maximum efficiency of the entire complex, bringing together form and function, combining the values of both to produce an efficient and responsive hospital model, achieving the optimization of all care processes at the service of users (patients, professionals and visitors).
The major challenge is to provide maximum functional precision within the proposed building volume, delivering an efficient, modern, sustainable design concept, based on the criteria of functional organization, segregation of circulations and routes, a solution that reflects contemporary values and the social importance of this type of building; the challenge is much more than just delivering a building, it is to provide a comprehensive response to a social need.
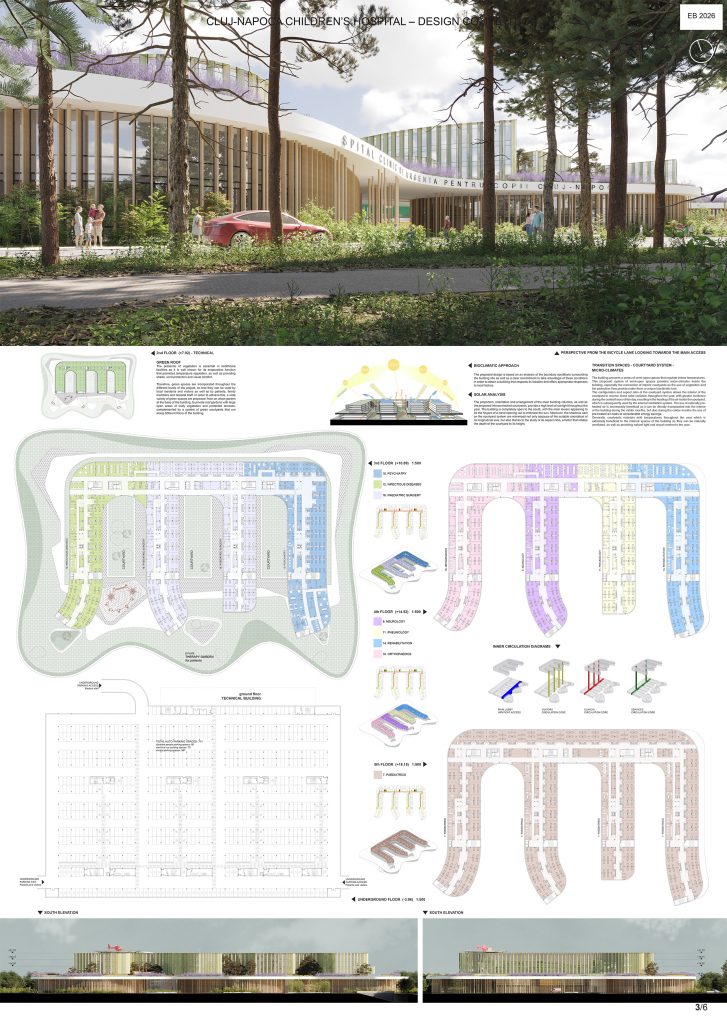
The volumetric concept of the hospital is based on a two floor base topped by a large overhanging green roof and a superior detached volume which overlooks the surrounding landscape, a model that we believe to be appropriate for the site and size of this hospital.
The model is simple and easily readable: while the base hosts the clinical and general services, the superior volume is dedicated to hospitalization. The hospital specialities are distributed in the four arms of the superior volume. A perfectly hierarchical and independent access system has been planned for outpatient, public, clinical and service uses, in addition to the specific ones for underground parking.
THE BUILDING
The building follows a deliberately simple layout.
The hospital base is structured in three well-differentiated functional areas:
The southern block accommodates the outpatient area, consisting mainly of a large double-height lobby, to which the outpatient areas (consultation, rehabilitation and administration) and the hospitalization visiting areas are connected.
The northern block hosts the clinical area which is divided in clinical use (on the first floor) and services (on the ground floor).
The intermediate area connecting the first two consists of 4 clinical blocks arranged perpendicularly to the previous ones and separated by spacious courtyards, which allow access either to outpatients (through the outpatient area), or to the medical staff (through the clinical area), depending on the needs.
A large roof with curved edges is placed on top of the base, providing open-spaces for leisure activities, games and walking for the children and their families, away from the public areas.
Hospitalization units are placed above the base, connected to the base through separated accesses: the clinical units with the clinical corridor on the lower floors, the service units also with the ground floor service corridor and the outpatients-visits with the main lobby.
The curved shapes of the outpatient areas, the base roof and the superior hospitalization volume respond to the additional challenge that a paediatric hospital poses, of being perfectly functional while having a playful appearance.
THE ACCESSES
Inside the building, the public access and circulation areas have been segregated from the clinical and service areas. In addition, the underground car park is directly connected to the main lobby by dedicated stairs and lifts, which act like functional connections of direct use, without sacrificing the rest of the vertical connections, especially in cases of evacuation needs. This means that, except for emergency evacuation needs, the car park is connected directly to the main lobby only, providing enhanced access control to the building.
Outside the building, the service, ambulatory, public and emergency accesses have been separated, as well as the 3 entrances to the car park. A perimeter alley integrated in the garden provides access to the fire brigade on all sides of the building.
Connections to the outside are provided by two major roundabouts that will absorb and channel traffic from the exterior.
BUILDING SERVICES
The general facilities have been separated from the main building, and placed in an adjacent independent volume, thus improving the safety and maneuverability in the area; one side of the street is planned as logistical access and the other as access to the facilities building. In addition to the above mentioned technical volume, a technical floor is placed between the two-floor base and the superior volume of the on the level of the green roof, housing sub-central units and air-conditioning equipment for highly specialized technical areas such as the surgical block and ICU. By implementing this technical floor, we are able to free the hospitalization volumes’ roof PV panels and improved heliport access.
THE COLOUR SCHEMES OF THE MAIN FACADE
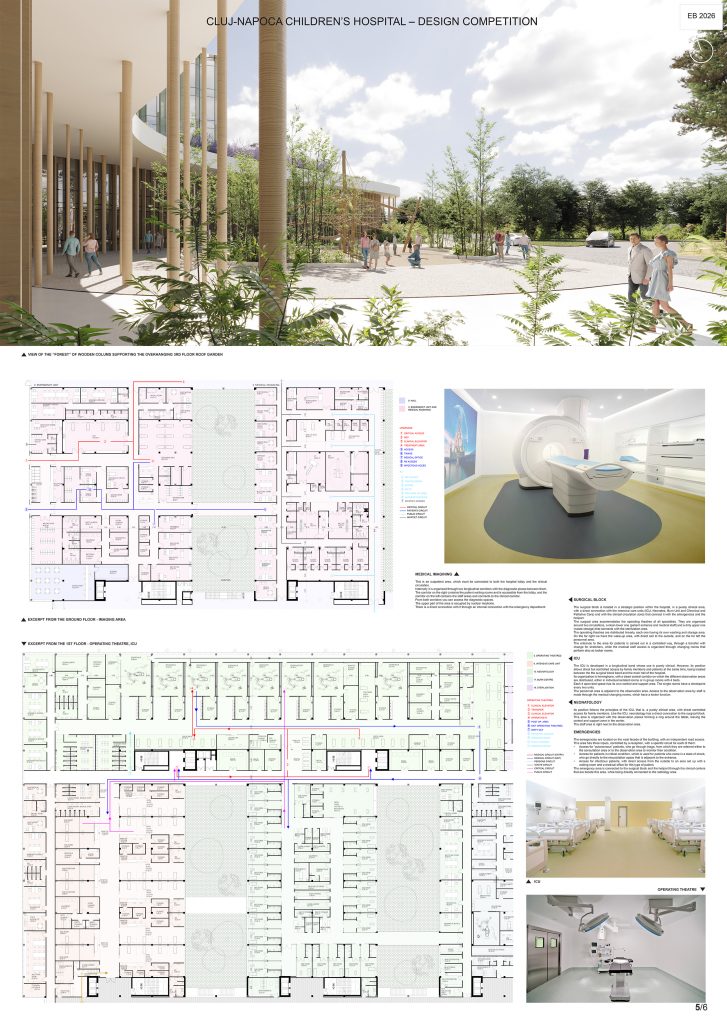
The overhanging green roof at the third level of the hospital is supported by slender wooden columns similar to high tree trunks. Entering the building through these columns into the main lobby would be like arriving in a clearing within the forest. This access concept helps to create a relaxing atmosphere for the children, when they approach the building.
The upper floors which host the hospitalization wards have transparent facades overlooking towards the surrounding landscape. Vertical fins of coloured translucent glass produce playful light hues within the rooms.
The chosen scheme is made of carefully selected colours like FLASHY GREEN, the color of abundance which relaxes and contributes to better health of kids, or INQUISITIVE YELLOW, the color of sunshine for children. Yellow is a color of mind and deep intellect, ideal for use in kids’ rooms, study rooms, and their play areas.
LOBBY / HALL
The lobby is the main entrance to the building, stretching along its entire width, between the outpatient area and the clinical area. In this place the exterior and interior spaces are blended in perfect continuity, integrating the organic volumes with the rest of the hospital.
In this double-height space, crossed by walkways at the first floor, all public accesses are channeled from three sides of the building: on the front the main visitors entrance, and treatment area access, to the east the teaching staff access and to the west the cafeteria access.
The main lobby brings together all the entrances to outpatient, hospitalization, teaching areas and underground parking area as follows:
Outpatient area: the rounded-shaped volumes that make up the outpatient consultations, admission and treatment unit on the ground floor, and nephrology and outpatient-unit on the first floor and the longitudinal medical imagining bands, blood transfusion unit and laboratory.
Hospitalization area: through the vertical cores inserted in the longitudinal bands, it is possible to access both the conventional hospitalization of the superior volume and the special units of ICU, Neonatology, Burn Unit and Palliative Unit that are on the first floor.
Research and Teaching area: it can be accessed directly from the outside or from the vehicle through the wind-shelter that regulates the flows to said area.
Parking: to prevent direct access to conventional hospitalization from the parking lot, specialized circulation cores are generated at the end of the interior courtyards, linking the underground parking with the lobby.
This area flooded with natural light can be configured as a multifunctional space where exhibitions, playgrounds, recreation areas can be developed. It contains commercial areas, chapel, resting and waiting areas.
The extended green roof above the second floor, combined with the curved shape of the outpatient volumes and the continuity of the pavement to the exterior, contributes to blurring the boundaries between interior and exterior.
SURGICAL BLOCK
The surgical block is located in a strategic position within the hospital, in a purely clinical area, with a direct connection with the intensive care units (ICU, Neonates, Burn Unit and Chronical and Palliative Care) and with the clinical circulation cores that connect it with the emergencies and the heliport.
The surgical area accommodates the operating theatres of all specialties. They are organized around two circulations, a clean lower one (patient entrance and medical staff) and a dirty upper one (waste storage) that connects with the sterilization area.
The operating theatres are distributed linearly, each one having its own washing and storage area. On the far right we have the wake-up area, with direct exit to the outside, and on the far left the personnel area.
The entrance to the area for patients is carried out in a controlled way, through a transfer with change for stretchers, while the medical staff access is organized through changing rooms that perform also as locker rooms.
ICU
The ICU is developed in a longitudinal band whose use is purely clinical. However, its position allows direct but controlled access by family members and patients at the same time, being located between the the surgical block band and the main hall of the hospital.
Its organization is herringbone, with a clean central corridor on which the different observation areas are distributed, either in individual isolated rooms or in group rooms with 4 beds.
Each 4 open-bed space has its own control and support area. The single rooms have a checkpoint every two units.
The personnel area is adjacent to the observation area. Access to the observation area by staff is made through the medical changing rooms, which have a locker function.
NEONATOLOGY
Its position follows the principles of the ICU, that is, a purely clinical area, with direct controlled access for family members. Like the ICU, neonatology has a direct connection to the surgical block.
This area is organized with the observation pieces forming a ring around the tablet, leaving the control and support zone in the center.
The staff area is right next to the observation area.
EMERGENCIES
The emergencies are located on the west facade of the building, with an independent road access.
This area has three inputs, controlled by a reception, with a specific circuit for each of them:
Access for “autonomous” patients, who go through triage, from which they are referred either to the consultation area or to the observation area to monitor their condition.
Access for patients in critical condition, which is used for patients who come in a state of shock, who go directly to the resuscitation space that is adjacent to the entrance.
Access for infectious patients, with direct access from the outside to an area set up with a waiting room and a medical office for this type of patient.
The emergency area is connected to the surgical block and the heliport through the clinical centers that are beside this area, while being directly connected to the radiology area.
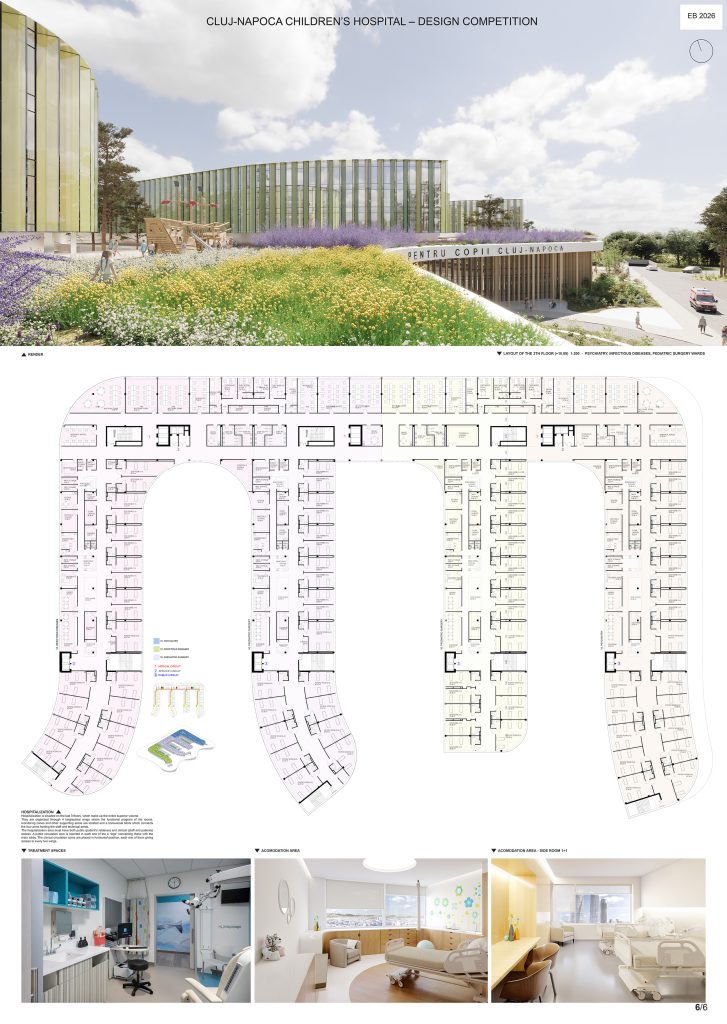
HOSPITALIZATION
Hospitalization is situated on the last 3 floors, which make up the entire superior volume.
They are organized through 4 longitudinal wings where the functional program of the rooms, monitoring zones and other supporting areas are located and a transversal block which connects the four arms hosting the staff and technical areas.
The hospitalization area must have both public (patient’s relatives) and clinical (staff and patients) access. A public circulation core is inserted in each one of the 4 “legs” connecting these with the main lobby. The clinical circulation cores are placed in horizontal position, each one of them giving access to every two wings.